.png)

ENDOMETRIOSIS & FERTILITY
What You Need to Know! Backed by Science
WHO | ASRM | ESHRE | Cochrane | SART | Adults 25+
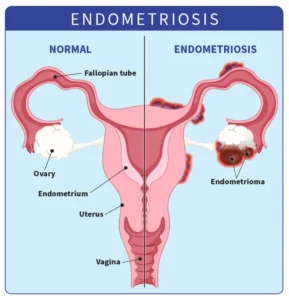
➤ What Is Endometriosis?
Endometriosis is a chronic inflammatory disease in which tissue similar to the uterine lining grows outside the uterus, most commonly on the ovaries, fallopian tubes, and peritoneum. Each menstrual cycle, this tissue bleeds internally, causing inflammation, adhesions, and often significant pain.
It affects 1 in 10 women of reproductive age, approximately 190 million people worldwide, yet diagnosis is delayed an average of 7 to 10 years. That diagnostic gap has real consequences for fertility.
➤ Symptoms to Watch For
- Painful periods: pain that disrupts daily life, not just discomfort
- Chronic pelvic pain: cyclical or persistent, inside or outside your period
- Pain during sex, urination, or bowel movements
- Heavy or irregular bleeding
- Fatigue, bloating, and gastrointestinal symptoms
- Difficulty getting pregnant: sometimes the only symptom
➤ Stages of Endometriosis
Endometriosis is classified into four stages by the ASRM based on the extent and location of lesions. Stage is a guide, not a verdict on your fertility potential.
➤ How Endometriosis Affects Fertility
Endometriosis impairs fertility through five overlapping mechanisms:
- Anatomical distortion: adhesions block or displace the tubes and ovaries
- Reduced ovarian reserve: endometriomas (ovarian cysts) damage healthy egg-producing tissue, lowering AMH
- Toxic peritoneal environment: inflammatory proteins impair sperm, egg quality, and embryo development
- Impaired uterine receptivity: altered implantation markers reduce embryo attachment success
- Lower oocyte quality: DNA fragmentation rates are higher in eggs from affected ovaries
➤ Diagnosis
Definitive diagnosis requires laparoscopy (minimally invasive surgery), but expert imaging is increasingly accurate for initial evaluation:
- Transvaginal ultrasound (TVUS): highly effective for endometriomas and deep disease in specialist hands
- MRI: detailed mapping for complex or pre-surgical cases
- Laparoscopy: gold standard; also allows simultaneous surgical treatment
If you suspect endometriosis, seek referral to a gynecologist or reproductive endocrinologist with specialist expertise in this condition.
➤ Fertility Treatment Options
➜ Expectant Management
For Stage I–II disease in patients under 35 with open tubes, natural conception attempts for 6–12 months are appropriate. Monthly fecundity rates are 2–4% (vs. 15–20% in unaffected couples).
➜ Ovulation Induction + IUI
Letrozole-based ovulation induction combined with IUI improves per-cycle rates to ~9–11% in mild disease with patent tubes. Three to six cycles before escalating to IVF is standard.
➜ Laparoscopic Surgery
A Cochrane meta-analysis (Jacobson et al., 2010) confirms that surgical removal of Stage I–II lesions significantly improves spontaneous pregnancy rates. For endometriomas, removal improves IVF access but carries a risk of reducing ovarian reserve — requires careful individualized decision-making.
➜ IVF / ICSI
The most effective option for Stage III–IV disease or failed prior treatments. IVF bypasses the pelvic environment entirely, retrieving multiple eggs and optimizing embryo selection. Live birth rates for women under 35 with endometriosis: 30–40% per cycle at accredited centers (SART, 2022).
➜ Egg Freezing, Fertility Preservation
For those not yet ready to conceive, proactive egg freezing is strongly recommended by ASRM and ESHRE. Endometriosis is progressive; banking eggs at a younger age preserves future options before reserve declines further.
A Note for Partners
Perceived partner support is one of the strongest protective factors against fertility-related psychological distress (Schmidt et al., 2005). Learning about endometriosis, attending appointments, and being present matters clinically as much as emotionally. Partners should also have their own fertility assessed, male factor infertility is present in 40–50% of couples experiencing difficulty conceiving.
Questions to Ask Your Specialist
- What stage is my endometriosis, and what does it mean for my fertility timeline?
- Has my ovarian reserve been tested (AMH + antral follicle count)
- Should I have surgery before trying to conceive — and what is the risk to my reserve
- Is IUI appropriate, or should we go directly to IVF?
- Should I consider egg freezing now, given the progressive nature of this disease?
- Can you refer me to a fertility counselor?
Key References
WHO, 2023 | ASRM Committee Opinion, 2022 | ESHRE Guideline 4th Ed., 2022 | Jacobson et al., Cochrane 2010 | Raffi et al., Human Reproduction 2012 | Lessey & Young, Fertility and Sterility 2019 | SART National Summary Report 2022 | Schmidt et al., Human Reproduction 2005