.png)
Recurrent miscarriage & what science knows
Raghad Altoubah- Reproductive & Fertility Medical Writer

REPRODUCTIVE HEALTH EDUCATION
Recurrent Miscarriage: What Science Knows
Evidence-based answers for people navigating pregnancy loss and what comes next.
Losing a pregnancy once is devastating. Losing two or more in a row can make you question whether parenthood will ever be possible.
Recurrent miscarriage, defined by most leading medical bodies as two or more consecutive pregnancy losses affects roughly 1 in 50 couples trying to conceive. You are not alone, and you are not without options.
This article explains what the science currently understands about why recurrent miscarriage happens, what investigations are recommended, and what treatments have real evidence behind them.
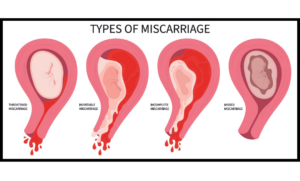
What Counts as Recurrent Miscarriage?
Medical definitions have evolved. The European Society of Human Reproduction and Embryology (ESHRE) now defines recurrent pregnancy loss (RPL) as two or more failed pregnancies confirmed by ultrasound or histology before 24 weeks gestation.
The American Society for Reproductive Medicine (ASRM) uses a similar threshold.
The shift from the older “three losses” definition to two losses reflects a growing recognition that couples deserve investigation and support earlier, not after a third heartbreak.
“Statistically, about 50–75% of all miscarriages are caused by chromosomal abnormalities in the embryo, a one-time event with no bearing on future pregnancies. But in recurrent cases, an underlying cause can be found in approximately 50% of couples.” — ESHRE Guideline on Recurrent Pregnancy Loss, 2023
Known Causes: What Science Has Identified
Research points to several well-established contributing factors:
➜ Genetic & Chromosomal Factors
- Chromosomal errors in the embryo account for the majority of individual miscarriages and remain the most common cause in recurrent cases too.
- Around 2–5% of couples with recurrent miscarriage carry a balanced chromosomal rearrangement (such as a translocation) that can be passed to embryos in an unbalanced form.
- Preimplantation genetic testing for aneuploidies (PGT-A) may improve live birth rates for couples with identified chromosomal causes, though this is still an area of active research.
➜ Uterine Abnormalities
- Structural issues in the uterus: such as a septum (a wall dividing the uterine cavity), fibroids that distort the cavity, or adhesions (scar tissue) are found in 10–15% of women with recurrent miscarriage.
- A uterine septum is the most common correctable structural anomaly. Surgical removal (hysteroscopic resection) is recommended by ESHRE when a septum is confirmed, though more data are needed on the exact benefit.
➜ Antiphospholipid Syndrome (APS)
- APS is one of the most important treatable causes of recurrent miscarriage. It is an autoimmune condition in which abnormal antibodies increase the risk of blood clots and pregnancy loss.
- Women with APS and recurrent miscarriage have significantly improved outcomes when treated with low-dose aspirin and low-molecular-weight heparin (LMWH) during pregnancy. This is one of the strongest evidence-based interventions available.
➜ Hormonal & Metabolic Factors
- Thyroid disorders (both underactive and overactive thyroid) are associated with pregnancy loss. Testing and treatment are recommended for any woman with recurrent miscarriage.
- Polycystic ovary syndrome (PCOS) has been linked to higher miscarriage rates, though the mechanism is not fully understood.
- Uncontrolled diabetes and some other metabolic conditions can also contribute.
➜ The Male Factor
Research increasingly shows that sperm quality matters beyond just achieving fertilisation.
High levels of DNA fragmentation in sperm are associated with higher miscarriage rates.
Testing for sperm DNA fragmentation is now discussed in many RPL clinics, though the best management approach is still being studied.
➜ Unexplained Recurrent Miscarriage
Even after thorough investigation, around 50% of couples will not receive a definitive explanation. This is understandably difficult to hear. But importantly, the outlook is still hopeful. Studies show that approximately 65–75% of couples with unexplained recurrent miscarriage will go on to have a successful pregnancy — particularly with supportive care and monitoring.
What Investigations Should You Expect?
ESHRE and ASRM guidelines recommend the following tests as part of a standard recurrent miscarriage work-up:
- Karyotyping of both partners (blood test to check chromosomes)
- Uterine assessment : via ultrasound, hysteroscopy, or MRI
- Antiphospholipid antibody testing (lupus anticoagulant, anticardiolipin, anti-beta2 glycoprotein)
- Thyroid function tests (TSH, and anti-thyroid antibodies)
- Fasting glucose and HbA1c (to screen for diabetes)
- Semen analysis and sperm DNA fragmentation testing, increasingly recommended
Thrombophilia testing beyond APS remains controversial. Currently, there is insufficient evidence that inherited thrombophilias (such as Factor V Leiden) cause recurrent miscarriage or that treating them improves outcomes. Your doctor should guide you based on your individual history.
Treatments with Evidence
- For APS: Aspirin + LMWH heparin
- For thyroid disorders: Thyroid hormone replacement or treatment
- For uterine abnormalities: Hysteroscopic surgery to correct a uterine septum or remove submucosal fibroids
- For chromosomal causes: Preimplantation genetic testing (PGT-A) in IVF, for couples with chromosomal rearrangements
- Progesterone: Progesterone supplementation in early pregnancy has shown benefit in women with recurrent miscarriage who experience early pregnancy bleeding, based on the large PRISM trial (UK).
Treatments NOT currently supported by evidence:
- Immunotherapy (intravenous immunoglobulin, lymphocyte immunotherapy, TNF-alpha blockers), currently not recommended outside of clinical trials.
- Routine use of anticoagulants for inherited thrombophilias without APS.
- Many supplements marketed for miscarriage prevention lack clinical trial data.
The Emotional Reality
Recurrent pregnancy loss is a grief that often goes unacknowledged by the world around you. Research consistently shows high rates of anxiety, depression, and post-traumatic stress among people who experience it and this is true for both partners.
Psychological support, whether through individual counselling, couples therapy, or specialist support groups, is now considered an integral part of recurrent miscarriage care by ESHRE. This is not a “nice to have.” It is part of evidence-based treatment.
If you are struggling emotionally after pregnancy loss, please reach out to your healthcare provider. Many RPL clinics now offer or can refer you to dedicated psychological support.
Key Takeaways
- Recurrent miscarriage (2+ losses) affects 1–2% of couples, investigation should begin after two losses.
- A cause is found in about 50% of cases; the most important treatable cause is antiphospholipid syndrome.
- Even without a clear cause, most couples will achieve a successful pregnancy.
- Both partners should be investigated, male factors matter.
- Be cautious of unproven treatments. If something sounds too good, ask your doctor for the evidence.
This article is for educational purposes only and does not replace personalised medical advice. Please speak with a qualified reproductive medicine specialist for assessment and treatment.