.png)

THYROID HEALTH & FERTILITY
What Every Person Trying to Conceive Should Know
Evidence-based patient education | Reviewed against ESHRE, ATA, and WHO guidelines
Your thyroid is a small, butterfly-shaped gland in your neck! But its influence on reproductive health is enormous.
Thyroid hormones Regulate Metabolism, Ovulation, Sperm production, and Fetal development. Even subtle imbalances that cause no obvious symptoms can quietly interfere with conception and increase the risk of miscarriage.
The good news: thyroid disorders are among the most treatable causes of fertility problems. Getting tested, diagnosed, and properly managed can make a meaningful difference, for both women and men.
How the Thyroid Affects Fertility
The thyroid produces two key hormones: Thyroxine (T4) and Triiodothyronine (T3) regulated by thyroid-stimulating hormone (TSH) from the pituitary gland.
These hormones interact directly with the reproductive system in several ways:
➜ In Women
- Disrupted menstrual cycles: Both hypothyroidism and hyperthyroidism can cause irregular, absent, or very heavy periods, making it harder to time conception.
- Impaired ovulation: Thyroid imbalance affects the hormones that trigger ovulation (LH and FSH), potentially preventing egg release altogether.
- Reduced egg quality: Thyroid hormones play a role in follicle development and the maturation of eggs.
- Higher miscarriage risk: Untreated hypothyroidism, particularly with elevated TSH, is associated with increased rates of early pregnancy loss.
- Complications in pregnancy: Thyroid disorders, if unmanaged, raise the risk of preeclampsia, preterm birth, and low birth weight.
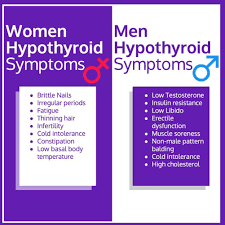
➜ In Men
- Sperm quality: Thyroid hormones are involved in sperm production and maturation. Both hypothyroidism and hyperthyroidism have been linked to reduced sperm count, poor motility, and abnormal morphology.
- Sexual function: Thyroid imbalance can contribute to reduced libido and erectile dysfunction.
- Testosterone levels: Thyroid disorders can alter sex hormone balance in men, affecting overall reproductive function.
The Two Main Thyroid Conditions That Affect Fertility
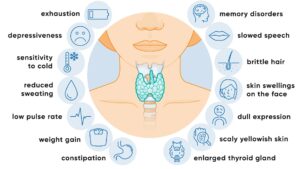
➜ Hypothyroidism (Underactive Thyroid)
Hypothyroidism is the most common thyroid disorder linked to fertility problems.
The thyroid does not produce enough hormones, slowing bodily processes. The most frequent cause is Hashimoto’s thyroiditis, an autoimmune condition in which the immune system attacks the thyroid gland.
Many people with mild hypothyroidism have no noticeable symptoms at all which is why blood testing is essential for anyone struggling to conceive.
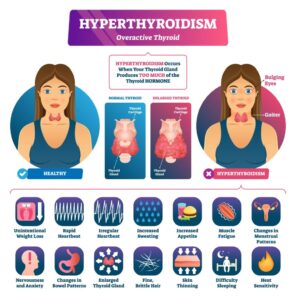
➜ Hyperthyroidism (Overactive Thyroid)
Hyperthyroidism occurs when the thyroid produces too much hormone, speeding up metabolism. The most common cause is Graves’ disease, another autoimmune condition.
What About Thyroid Antibodies?
Even when TSH levels appear normal, the presence of thyroid antibodies, particularly anti-thyroid peroxidase (anti-TPO) antibodies, may affect fertility and pregnancy outcomes.
Research published in peer-reviewed fertility journals, and referenced in ESHRE guidelines, suggests that women with elevated thyroid antibodies and otherwise normal thyroid function have higher rates of miscarriage and may respond less well to IVF.
The mechanism is not fully understood, but immune dysregulation is thought to play a role.
Testing for thyroid antibodies is now recommended for women undergoing fertility treatment, even if their TSH is within range.
Getting Tested: What to Ask For
A standard thyroid panel for fertility evaluation should include:
- TSH (thyroid-stimulating hormone): The primary screening test. For people trying to conceive, most reproductive endocrinologists recommend a TSH below 2.5 mIU/L — a tighter range than general population guidelines.
- Free T4 (FT4): Measures the active thyroid hormone circulating in the blood.
- Free T3 (FT3): Sometimes included, especially if symptoms persist despite normal TSH.
- Anti-TPO antibodies: Recommended for anyone with fertility concerns or a history of miscarriage.
- Anti-thyroglobulin (anti-TG) antibodies: Sometimes tested alongside anti-TPO.
Speak with your doctor or reproductive endocrinologist about which tests are appropriate for your situation. If you have a history of thyroid disease, autoimmune conditions, or recurrent miscarriage, comprehensive testing is especially important.
Treatment and Fertility Outcomes
➜ Treating Hypothyroidism
Hypothyroidism is treated with levothyroxine, a synthetic form of T4 taken once daily. It is safe, well-tolerated, and highly effective. Achieving a TSH within the recommended preconception range (generally below 2.5 mIU/L) is associated with improved fertility outcomes, including better IVF success rates and reduced miscarriage risk.
Dosage requirements increase during pregnancy, so close monitoring every 4–6 weeks in the first trimester is standard practice.
➜ Treating Hyperthyroidism
Treatment options include antithyroid medications (such as methimazole or propylthiouracil), radioactive iodine therapy, or surgery. The choice depends on the severity of disease, underlying cause, and whether pregnancy is planned in the near term. Some treatments require a waiting period before conception. Your endocrinologist will guide the timing.
➜ Subclinical Hypothyroidism
Subclinical hypothyroidism — defined as a mildly elevated TSH with normal T4 — is a more nuanced area. Evidence from major guidelines (ATA, ESHRE) supports treatment with low-dose levothyroxine for women who are pregnant, trying to conceive, or undergoing IVF, particularly when antibodies are also present.
When to See a Specialist
Consider asking for a thyroid evaluation if you:
- Have been trying to conceive for 6–12 months without success
- Have experienced one or more miscarriages
- Have irregular periods or signs of ovulation problems
- Have a personal or family history of thyroid disease
- Have been diagnosed with an autoimmune condition
- Are planning IVF or another form of assisted reproduction
- Are experiencing symptoms consistent with thyroid imbalance
Your primary care physician can order initial thyroid testing.
For complex fertility cases, a reproductive endocrinologist (fertility specialist) and an endocrinologist may work together to optimize your thyroid health before and during treatment.
Key Takeaways
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.