
.png)
REPRODUCTIVE HEALTH EDUCATION
Fibroids: When They Matter
What every person with a uterus should know and when to seek care
Medically reviewed | Evidence-based | Sources: WHO, ACOG, ESHRE
Uterine fibroids are among the most common benign (non-cancerous) conditions affecting people with a uterus. By age 50, up to 70–80% of women will have developed at least one fibroid! yet many will never know.
That is because most fibroids are silent. The real question is not whether you have them, but whether they are causing harm.
This guide answers the questions that matter most: What are fibroids? When do they need treatment? And what does the latest evidence say about your options?
➤ What Are Uterine Fibroids?
Fibroids also called “Uterine leiomyomas” or “Myomas“: are growths made of muscle and fibrous tissue that develop in or around the uterus. They are almost never cancerous (malignant transformation occurs in fewer than 1 in 1,000 cases).
They vary enormously in size: from a tiny seed to, in rare cases, the size of a grapefruit.
A person may have one fibroid or several at the same time.
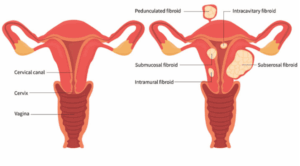
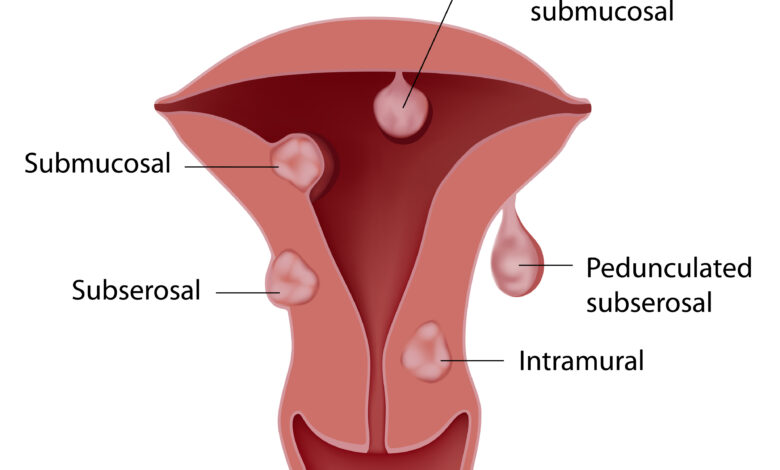
➤ Types of Fibroids
Where a fibroid grows inside or around the uterus determines how likely it is to cause symptoms:
Submucosal fibroids, though less common, tend to cause the most significant symptoms because they directly affect the uterine lining.
➤ Who Is at Risk?
Fibroids can develop in anyone with a uterus, typically between the ages of 30 and 50. Certain factors increase the likelihood:
- Race and ethnicity: Black women are 2–3 times more likely to develop fibroids than white women, and tend to develop them earlier and with greater severity (ACOG, 2022).
- Family history: Having a first-degree relative with fibroids significantly raises your risk.
- Early onset of periods: Starting menstruation before age 10 is associated with higher fibroid risk.
- Obesity: Higher body weight increases estrogen exposure, which can promote fibroid growth.
- Diet: Diets high in red meat and low in green vegetables and fruit have been associated with increased fibroid risk (WHO, 2023).
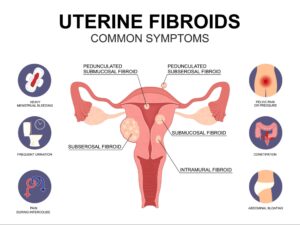
➤ Symptoms: How Do You Know When They Matter?
Most fibroids are asymptomatic and discovered incidentally during a routine ultrasound. However, when symptoms do occur, they can significantly affect quality of life. Common symptoms include:
- Heavy menstrual bleeding (menorrhagia): soaking through pads or tampons every hour for several hours
- Prolonged periods lasting more than 7 days
- Pelvic pressure, bloating, or a feeling of fullness
- Frequent urination or difficulty emptying the bladder
- Constipation or rectal pressure
- Pain during sex (dyspareunia)
- Lower back or leg pain
- A visibly enlarged abdomen
Heavy bleeding is the most common reason people seek help. Prolonged blood loss can lead to iron-deficiency anemia, causing fatigue, shortness of breath, and reduced concentration, symptoms that are often wrongly attributed to other causes.
➤ Fibroids and Fertility: What the Evidence Says
Most women with fibroids conceive and carry pregnancies without complications. However, the location and size of fibroids matter considerably for fertility.
According to ESHRE guidelines (2023), submucosal fibroids that distort the uterine cavity are associated with reduced implantation rates and higher miscarriage risk in both natural conception and IVF. Removing these fibroids (hysteroscopic myomectomy) has been shown to improve reproductive outcomes.
Intramural and subserosal fibroids generally have less impact on fertility, though large intramural fibroids (>4–5 cm) affecting the cavity may warrant evaluation before fertility treatment.
➤ Diagnosis: How Are Fibroids Found?
Fibroids are most commonly diagnosed through:
- Pelvic ultrasound (transvaginal or abdominal): the standard first-line investigation
- Sonohysterography: ultrasound combined with saline fluid to assess the uterine cavity
- MRI: used for complex cases, pre-surgical planning, or when ultrasound findings are inconclusive
- Hysteroscopy: direct visualization inside the uterine cavity, especially for submucosal fibroids
➤ Treatment Options: A Range of Choices
Not every fibroid needs treatment. The goal is to manage symptoms and protect fertility goals not to remove every fibroid detected. Decisions are guided by symptom severity, fibroid size and location, age, and whether pregnancy is desired.
1. Watchful Waiting
For fibroids that are asymptomatic and not affecting fertility, regular monitoring with pelvic ultrasound every 6–12 months is often all that is needed. particularly as menopause approaches, when fibroids naturally shrink.
2. Medical Management
- Hormonal contraceptives (pills, hormonal IUD): help manage heavy bleeding, do not shrink fibroids
- GnRH agonists (e.g., leuprolide): temporarily reduce fibroid size by lowering estrogen; used pre-operatively or for short-term symptom relief
- GnRH antagonists (e.g., elagolix, relugolix): newer oral agents approved for fibroid-associated heavy bleeding with demonstrated efficacy in clinical trials (ACOG, 2023)
- Tranexamic acid & NSAIDs: reduce bleeding volume and pain during menstruation
- Iron supplementation: essential if anemia is present
3. Minimally Invasive Procedures
- Uterine Fibroid Embolization (UFE): blocks blood supply to fibroids, causing them to shrink uterus is preserved
- Hysteroscopic myomectomy: surgical removal of submucosal fibroids via the vagina, no incision required
- Laparoscopic or robotic myomectomy: keyhole removal of intramural or subserosal fibroids
- MRI-guided focused ultrasound (MRgFUS): non-invasive treatment using sound waves to destroy fibroid tissue
4. Surgery
- Abdominal myomectomy: open surgery for large or multiple fibroids, preferred when fertility preservation is the goal
- Hysterectomy: complete removal of the uterus, the only permanent cure, reserved for those who have completed childbearing and have severe symptoms
➤ A Note on Disparities in Care
Research consistently shows that Black women experience disproportionate delays in fibroid diagnosis and are more likely to undergo hysterectomy rather than uterus-sparing procedures, even when less invasive options exist. Awareness, early access to specialist care, and patient advocacy are critical to closing this gap.
If you feel your symptoms are being dismissed or you are not being offered all available options, you have the right to ask questions and seek a second opinion.
➤ Key Takeaways
- Fibroids are extremely common and usually benign, most require no treatment
- Symptoms, not size alone, guide treatment decisions
- Heavy periods, pelvic pain, and difficulty conceiving are the most important signs that fibroids may need attention
- Multiple treatment options exist, and uterus-preserving treatments are available for those who want to remain fertile
- Early diagnosis and specialist referral improve outcomes significantly
This article is intended for public health education. It does not replace personalised medical advice. Always consult a qualified healthcare provider about your individual situation.



