.png)
PCOS: Facts vs. Social Media Myths
Raghad Altoubah- Reproductive & Fertility Medical Writer
PCOS: Facts vs. Social Media Myths | Evidence-Based Health Information
PCOS: Facts vs. Social Media Myths
What the science actually says and why it matters for your health
Scroll through any social media feed and you will find no shortage of PCOS “advice”, detox teas, miracle diets, and confident claims that your hormones are broken. Some of it sounds almost scientific. Most of it is not.
Polycystic Ovary Syndrome (PCOS) is the most common hormonal condition affecting people with ovaries worldwide, impacting an estimated 1 in 10 women of reproductive age (WHO, 2023). Yet despite how widespread it is, it remains one of the most misunderstood conditions in women’s health and social media has made the confusion worse.
➤ First, What Exactly Is PCOS?
PCOS is a hormonal and metabolic condition diagnosed when at least two of the following three criteria are present (Rotterdam Criteria, 2003):
- Irregular or absent menstrual cycles
- Elevated androgen levels (such as testosterone) detected by blood test or physical signs like acne and excess hair growth
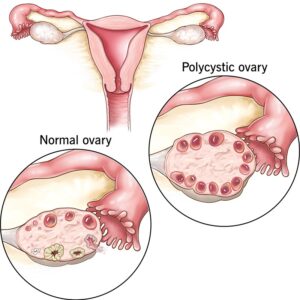
- Polycystic-appearing ovaries on ultrasound
Notice what that definition does not say: it does NOT require weight gain, infertility, or any particular diet failure. PCOS is a spectrum, two people with the same diagnosis can have very different symptoms and experiences.
➤ Myths vs. Facts: The Side-by-Side You Need
These are the most persistent PCOS myths circulating online today — and what the evidence actually shows.

➤ Why Getting This Right Matters
PCOS is not just a reproductive condition. Left unmanaged, it carries real long-term health implications:
- Up to 70% of people with PCOS have insulin resistance, a major driver of type 2 diabetes risk
- Increased risk of endometrial hyperplasia from chronic anovulation
- Higher prevalence of anxiety and depression compared to the general population
- Elevated risk of cardiovascular disease over the long term
This is not meant to alarm you! it is meant to underscore why an accurate diagnosis and a real management plan beat a detox tea every single time.
➤ What Actually Helps! Evidence-Based Management
There is no cure for PCOS, but its symptoms are highly manageable. Evidence-based approaches include:
The Bottom Line
PCOS is real, common, and complex. It is not your fault, it is not caused by eating too much sugar, and it is not a life sentence of infertility or ill health.
What it does require is accurate information, an honest conversation with a qualified clinician, and where relevant! a long-term management plan tailored to your specific goals. Whether that goal is regulating your cycle, managing metabolic risk, or starting a family, the science is on your side.
The best thing you can do right now? Close the wellness influencer tab, and open a conversation with your doctor.
This article is intended for informational purposes only and does not constitute medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.